SUBMIT YOUR MANUSCRIPT
Affiliations
ABSTRACT
An osteoid osteoma is a small non-malignant osteoblastic tumour with characteristic radiological finding of central lucent nidus with surrounding sclerosis typically presenting as non-traumatic night pain relieved by taking Non-Steroidal Anti-Inflammatory Drugs (NSAIDs). Atypical cases without the cardinal symptoms and different radiological findings can pose diagnostic challenges and result in delayed treatment. Here, we report a rare case of painless osteoid osteoma as an incidental finding in a 60-year-old male presenting for Magnetic Resonance Imaging (MRI) for evaluation of suspected lesion on x-ray, emphasising the importance of considering this rare variant. Since the lesion was too small and asymptomatic, the biopsy was not done and the diagnosis was made on the characteristics findings on x-ray, CT, and MRI.
Key Words: Osteoid osteoma, Atypical, Scaphoid bone.
INTRODUCTION
An osteoid osteoma is a non-malignant primary bone lesion that was first described by Jaffe in 1935.1
It is a benign osteoblastic, slowly progressive tumour which is usually less than 1.5 cm. It occurs mainly in adolescents and adult males, and is rarely found after 40 years.2,3
Osteoid osteoma typically presents as a central area of calcified osteoid tissue within a surrounding lucent area consisting of loose vascular connective tissue called nidus with surrounding sclerotic rim representing inflammatory reaction.
It presents more commonly in the long bones of lower extremity (>50%) and spine (10-15%), and less commonly in hands (6-13%). Most commonly involved bones in hand are proximal phalanx and scaphoid bones.1
However, the lesions in hand bones may present differently without the cardinal symptoms and can mimic tenosynovitis or other common wrist problems. Such atypical presentation of osteoid osteoma without hallmark symptoms can pose diagnostic challenges and result in delayed management.
CASE REPORT
A 60-year gentleman presented with non-specific right index finger pain for one year and difficulty in grip. He denied any history of trauma or recent illness or pain in the wrist joint.
On physical examination, there were no signs of swelling, erythema or tenderness at wrist joint. The x-ray of hand was done which was normal along the phalanges but there was an incidental finding of a rounded lucent area with central sclerotic dot along the anterior half of the scaphoid bone suspicious for osteoid osteoma (Figure 1). So, a CT scan of hand was done which showed features similar to x-ray with a lucent rounded area with central sclerotic dot (Figure 2). On MRI, it showed peripheral abnormal isointense area, which appeared lucent on radiograph and central low signal, which appeared sclerotic on radiograph (Figure 3). On the basis of the three imaging modalities, a diagnosis of osteoid osteoma was made.
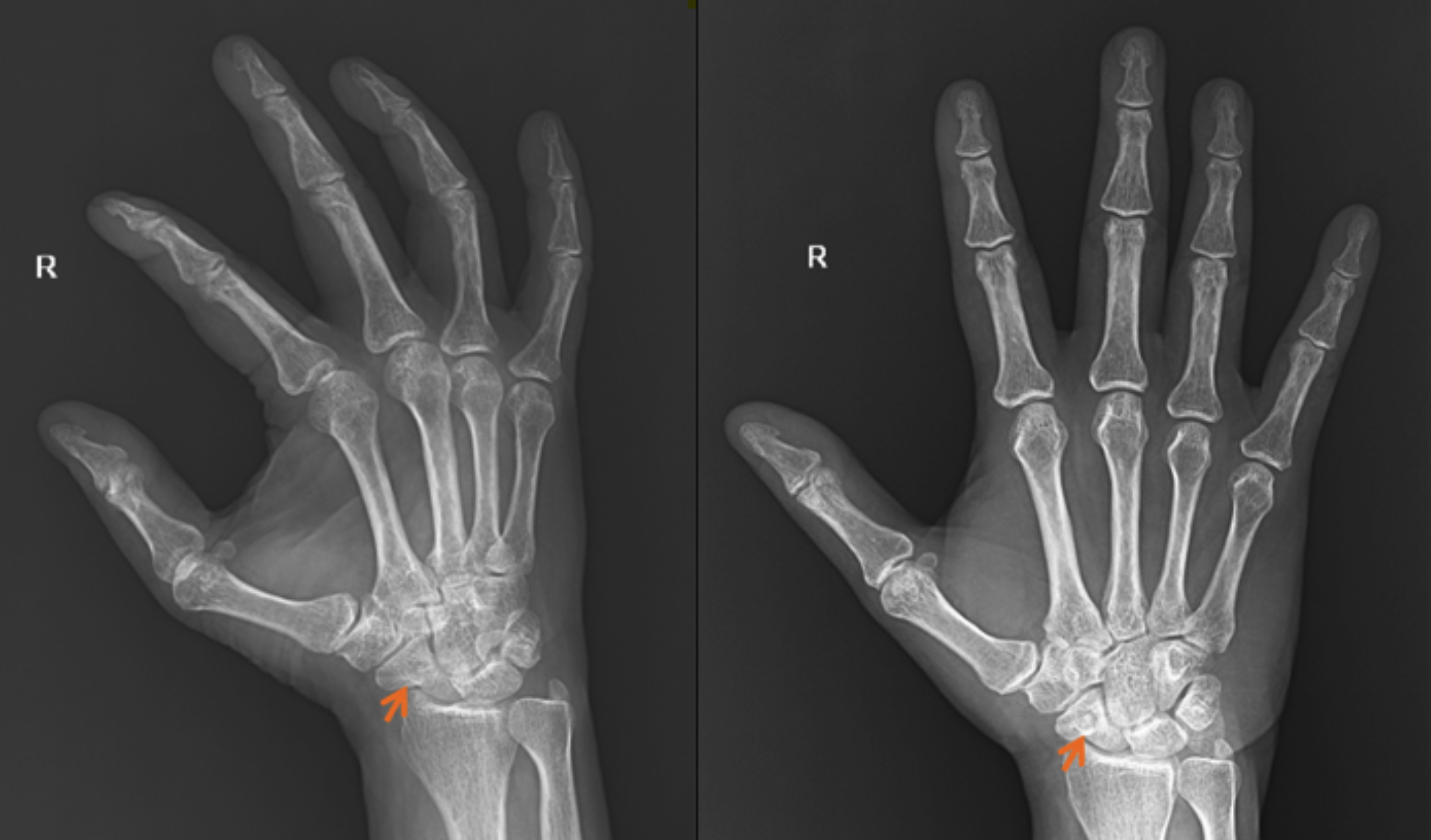 Figure 1: X-ray of the right of the hand. A small round lucent lesion with central nidus seen in the scaphoid bone (orange arrow). (a) Oblique view (b) Anteroposterior view.
Figure 1: X-ray of the right of the hand. A small round lucent lesion with central nidus seen in the scaphoid bone (orange arrow). (a) Oblique view (b) Anteroposterior view.
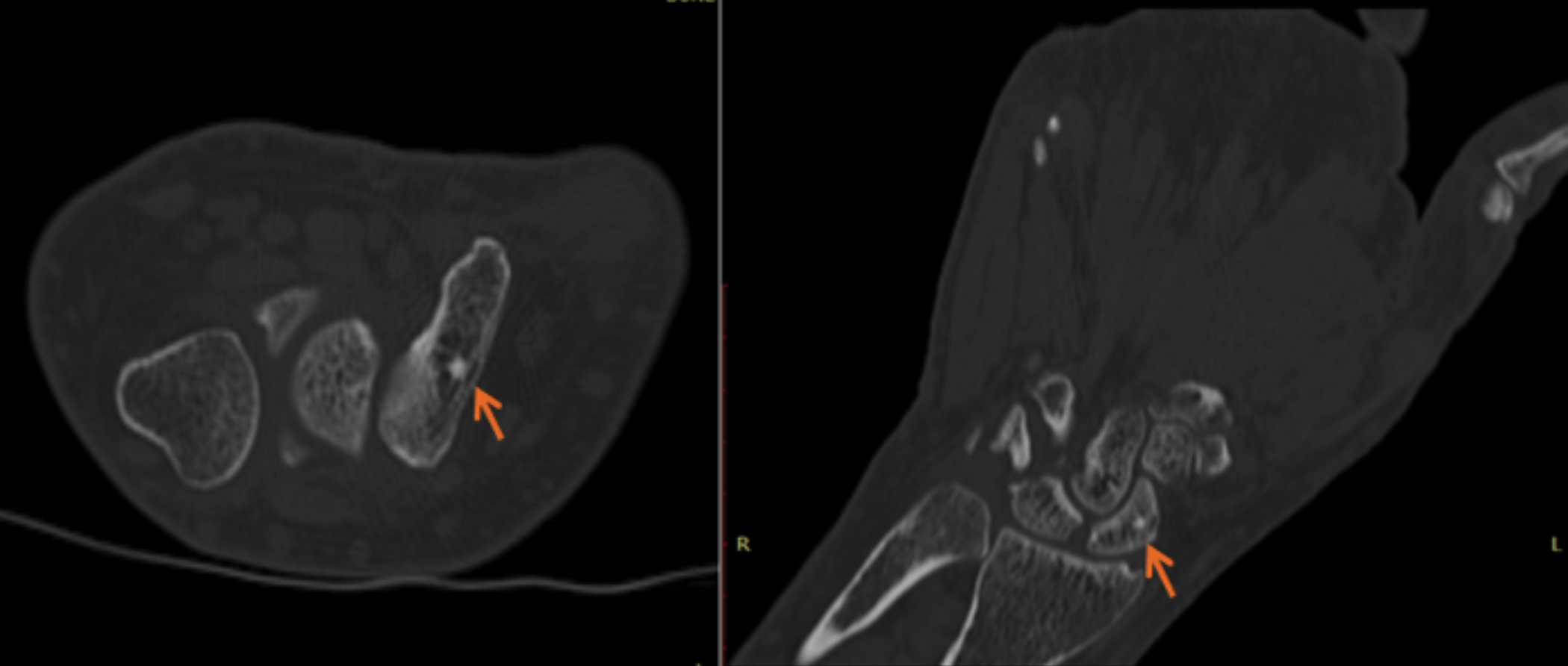 Figure 2: CT scan of the right hand (a) axial (b) coronal sections. A well-defined lucent area with central sclerotic focus representing nidus (arrows).
Figure 2: CT scan of the right hand (a) axial (b) coronal sections. A well-defined lucent area with central sclerotic focus representing nidus (arrows).
Figure 3: MRI of the right hand (a) cor STIR (b) 3D merge. A well-defined T2 hyperintense abnormal signal intensity area with central hypointense focus representing nidus (arrows).
DISCUSSION
Osteoid osteoma is a well-known benign bone tumour with typical presenting complaint of night pains that leads to its clinical diagnosis. However, painless osteoid osteomas have been reported. The exact reason for painless osteoid osteomas has not yet been known. However, a hypotheses was presented according to which absence of nerve fibers, peripheral location resulting in low body weight pressure and periosteal location may be the reasons behind it.4 Such atypical presentation of osteoid osteoma can result in delayed diagnosis and treatment, as painless lesions may not raise immediate suspicion.
Osteoid osteomas, which have different radiologic and clinical features, are called atypical osteoid osteomas.1 The diagnosis and management are frequently difficult in these cases due to non-specific symptoms. Osteoid osteoma in the carpal bones is rare and manifests itself differently from other parts of the skeleton. Its misdiagnosis is common, and the patients are usually treated for tendinitis, synovitis or other diseases that are commonly seen in the wrist.1
On plain radiograph, osteoid osteoma typically presents as a central sclerotic dot within a surrounding lucent area called nidus.5
CT is a superior modality at distinguishing the lesion and is the modality of choice. It typically shows a small well-defined lucent lesion within surrounding sclerotic inflammatory changes within bone. A central sclerotic focus can be seen.5
The imaging features such as extensive adjacent bone marrow oedema, soft-tissue changes, difficulty in detecting the nidus, and lesion locations close to a joint (with reactive arthritis) may mislead the diagnosis of osteoid osteoma as aggressive neoplastic lesion by MR imaging.6,7 The signal intensity of the nidus is different on all sequences and so is the contrast enhancement of the lesion. Usually, the tumour exhibits low-to-intermediate signals on T1WI and heterogeneously hyperintense signals on T2WI and STIR sequences. Central sclerotic focus of calcification shows hypointense signals on both T1- and T2-weighted sequences.5 Tumour enhancement is variable; most lesions enhance diffusely as a result of their internal vascularity; however, a heterogeneous peripheral enhancement may be seen. MRI may also depict bone marrow oedema with surrounding soft tissue edematous changes.
In conclusion, atypical presentations or imaging findings may delay diagnosis of osteoid osteoma and consequently, its treatment.
PATIENTS’ CONSENT:
Informed consent was obtained from the patient.
COMPETING INTEREST:
The authors declared no competing interest.
AUTHORS’ CONTRIBUTION:
SD: Evaluated the incidental finding of lesion seen on x-ray hand done with unrelated complaints.
ZNS: Conducted the literature review and wrote the case report.
SAK: Finalised the manuscript.
All authors approved the final version of the manuscript to be published.
REFERENCES